Zimmer and Peacock support algorithm development for POC technologies for our clients. Part of the process is deciding on a threshold value for the POCT so that patients can be separated into groups with and without the disease of interest.
An example would be a sepsis point-of-care test (POCT) where the results are used for screening and separating patients with sepsis from those without so that treatment can be appropriately applied.
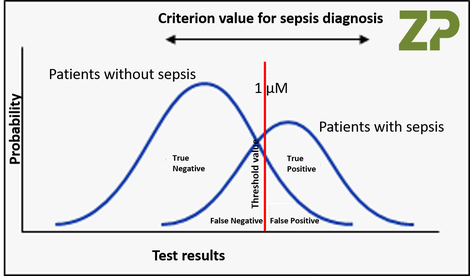
With any diagnostic there is a distribution in values for both the positive or negative results due to both the inherent variability with the technology but also within the patient groups, as everyone is unique. The question is how to choose a threshold value so that the algorithm can efficiently separate patients with sepsis from patients without, whilst maximising selectivity to avoid false positives and false negatives.
In the image opposite we have have applied an arbitrary value of 1 microM as the threshold value by which we will triage those with sepsis from those without sepsis; it can be seen that by moving the threshold value we increase or decrease the numbers true positives, true negatives, false positives and false negatives.
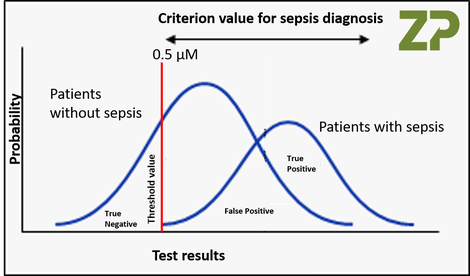
HIGH SENSITIVITY and LOW SELECTIVITY
In the adjacent image we have taken the same POCT, but increased it sensitivity. Here we have changed the threshold value to 0.5 microM, which captures all the positive results, which as states makes the test very sensitive, but The other effect of moving the threshold value to 0.5 microM is that it has increased the number of false positives which makes the test less selective, as it cannot efficiently separate the two patient groups.
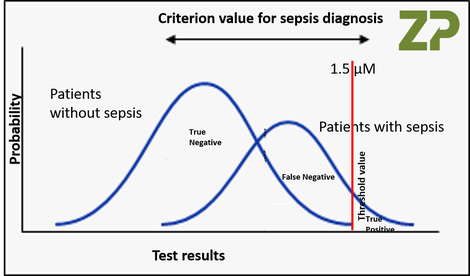
LOW SENSITIVITY and LOW SELECTIVITY
In the adjacent image we have moved the threshold value to 1.5 microM, which means we correctly identify all the patients without sepsis, but we only identify those patients with the highest value for sepsis when tested. With this threshold value the test has become both insensitive as it can only detect a small proportion of the patients with sepsis, and yet it is also unselective as it is not good at separating patients with and without sepsis.
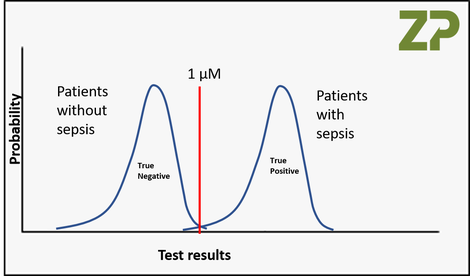
IDEAL WORLD
One could imagine an ideal POC Test which was so accurate and precise that it can easily distinguish between two patients groups with and without sepsis, we have illustrated this in the adjacent image. One would describe this diagnostic as both very sensitive and very selective around the threshold value of 1 microM.
In summary Zimmer and Peacock determine the threshold values as part of POCT development and manufacturing so as to maximise both the sensitivity and selectivity of the test, but we also weigh the clinical risks of false positives and false negatives.
Zimmer and Peacock are a pragmatic team of scientists and engineers, who take a holistic approach to sensor development and manufacturing programmes that we perform for our clients, please feel free to contact us to discuss your programme.